
























|
Getting your Trinity Audio player ready...
|
By: Mercura Wang
Colonoscopy is the most widely used screening test for colon cancer, which is the second leading cause of cancer-related death in the United States.
It is considered the gold standard and is more accurate than two other common screening methods—stool tests and sigmoidoscopy—because it allows doctors to see the entire colon and remove any potentially problematic polyps during the same procedure.
However, there is ongoing debate about who should undergo a colonoscopy and when. Not everyone will get colon cancer, and the procedure could lead to overdiagnosis as well as rare but serious side effects.
What Does a Colonoscopy Do?
The colon is the main part of the large intestine and is about 5 feet long in adults. The rectum stores stool until it passes through the anus. Together, they make up most of the large intestine, absorbing nutrients and converting liquid waste into solid stool.
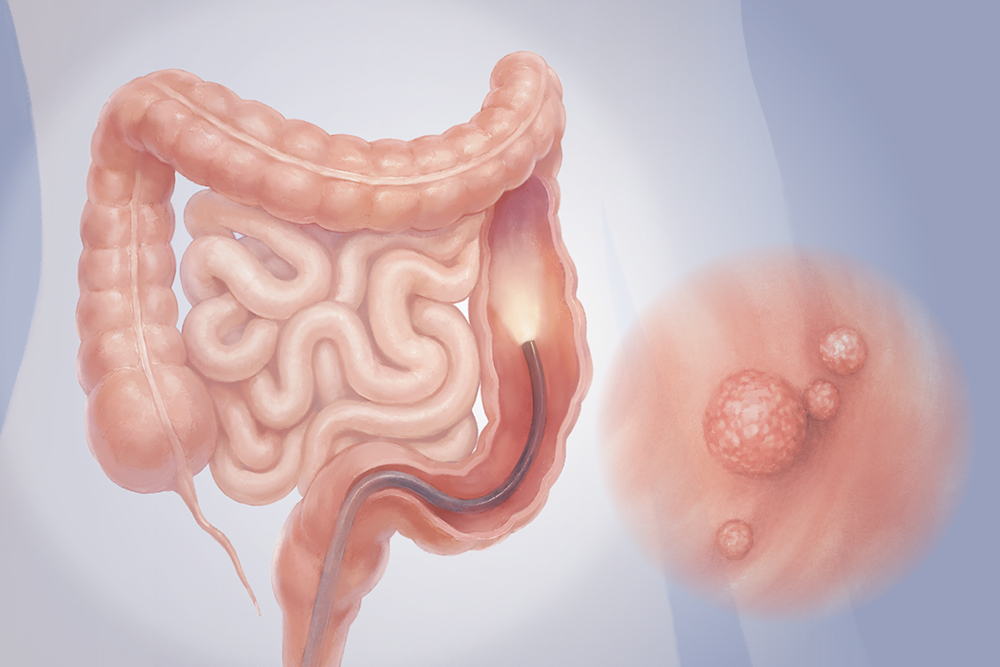
During a colonoscopy, a gastroenterologist inserts a thin, flexible tube with a lighted camera (colonoscope) through the anus to examine the lining of the rectum and colon. The tube introduces air to gently inflate the colon so the doctor can see more clearly. If polyps or other abnormalities are found, they can often be removed immediately using tools such as forceps, snares, or electrocautery devices passed through the scope.
The procedure takes about 20 to 45 minutes.
Most colonoscopies in the United States are performed under sedation or anesthesia, so patients may sleep through the entire procedure. Those who choose lighter sedation—or none at all—may feel some discomfort.
The primary purpose of colonoscopy is to prevent or detect colon cancer.
Beyond cancer screening, colonoscopy can be used to both detect and treat a range of problems in the colon and rectum, including polyps, ulcerations, and diverticula (small pouches that can form in the colon wall).
It can also help determine the underlying causes of symptoms such as chronic diarrhea, rectal bleeding, and changes in bowel habits. During the procedure, doctors can identify inflamed tissue, sources of bleeding, and other abnormalities in the colon.
Who Should Have a Colonoscopy, and When?
According to the current guidelines, colonoscopy is recommended for most adults starting at age 45, and repeated every 10 years if results are normal. More frequent screenings may be recommended depending on any abnormal findings.
People at higher risk are suggested to begin screening earlier—at age 40 or 10 years younger than the age at which a first-degree relative was diagnosed with colorectal cancer, whichever comes first.
In older adults, colonoscopy carries a greater risk of complications. After age 75, the decision to continue screening should be made in consultation with a doctor based on potential benefits, risks, and patient preferences.
Beyond the main guidelines, screening recommendations continue to evolve. For instance, some guidelines recommend initiating screening at age 50. In addition, emerging evidence suggests that follow-up intervals after a normal colonoscopy may be safely extended in some people. A 2024 study found that people without a family history of colorectal cancer and with an initial normal colonoscopy may be able to wait up to 15 years before repeat screening.
Some experts suggest weighing the benefits and risks. For a person with a family history of colon cancer, it may be beneficial to keep a close watch, while for someone at low risk, it may be a different story.
These differences highlight continuing uncertainty and the need for individualized clinical judgment as evidence continues to evolve.
In addition, colonoscopy may be avoided or require careful consideration in people who:
Have inadequate bowel preparation
Have a bowel perforation, severe inflammation, or infection
Have unstable health or significant medical conditions (advanced heart, lung, kidney, or liver disease)
Have a life expectancy of less than 10 years, or risks that outweigh the potential benefits
Have blood-clotting disorders
How Effective Is Colonoscopy?
“Colonoscopy has a sensitivity of 88 percent to 98 percent for identifying advanced, precancerous polyps,” Dr. Steven Lee-Kong, chief of colorectal surgery at Hackensack University Medical Center, told The Epoch Times.
The miss rate may be influenced by factors such as inadequate bowel preparation, the type of polyps being examined, and the skill of the endoscopist, noted Dr. Rucha Shah, a gastroenterologist. Small or flat polyps are harder to detect, and in some cases, the entire colon may not be fully visualized.
Colonoscopy allows doctors to remove precancerous polyps during the same procedure—something other screening tests cannot do. Removing these polyps has been shown to significantly reduce the risk of death from colorectal cancer, with one study reporting a 53 percent reduction in mortality associated with polyp removal.
However, recent studies have offered additional perspectives.
For example, colonoscopy is used much more frequently for screening in the United States than in Canada, where only about 15 percent of procedures are performed for screening, and most are diagnostic, yet colorectal cancer survival rates remain similar in both countries.
A major 2022 Nordic-European Initiative on Colorectal Cancer study found a modest reduction in colorectal cancer mortality with colonoscopy screening, no significant difference in overall death rates, and a low rate of serious complications.
What Are the Risks and Complications of Colonoscopy?
Colonoscopy is generally safe, but like all medical procedures, it carries some potential risks and complications. Most are minor and resolve quickly.
Gas, Bloating, Cramping, or Stomach Discomfort: These symptoms are mainly caused by air introduced during the exam and temporary changes in gut bacteria from the bowel preparation. These typically resolve within a day or two, although some people may notice symptoms lasting a few weeks.
Nausea, Vomiting, Dizziness, or Dehydration: These symptoms may occur as a result of the osmotic laxative used for bowel preparation.
Mild Redness or Tenderness at the IV Insertion Site: This may occur in the arm where the intravenous line was placed.
Medication Side Effects: Sedation or anesthesia may cause temporary changes in blood pressure, rash, or breathing difficulties.
Electrolyte Imbalances or Kidney Problems: In some cases, the bowel preparation may lead to low levels of potassium, sodium, or magnesium, or affect kidney function.
Less Common and More Serious Side Effects
Certain complications are directly related to the colonoscopy procedure itself.
Bleeding: Bleeding may occur after a biopsy or polyp removal, usually during or shortly after the procedure, although it can occasionally be delayed for up to one week. It is typically minor, with significant bleeding being rare and occurring in less than 1 percent of cases. The risk increases based on the size of the removed polyp.
Perforation: Perforation during colonoscopy is very rare (less than one in 1,Colonoscopy is the most widely used screening test for colon cancer, which is the second leading cause of cancer-related death in the United States. Credit: Illustration by The Epoch Times, Shutterstock procedures) and involves a tear in the intestinal wall that can allow bowel contents to leak into the abdomen, potentially causing infection. It may occur due to mechanical injury from the scope or instruments, overinflation of the bowel, or thermal damage during polyp removal. Symptoms typically include pain during or shortly after the procedure, although small perforations may appear later. Untreated cases can lead to fever and abdominal infection.
Postpolypectomy Syndrome: This occurs when heat from electrocoagulation (the removal of tissue with an electrical current) injures the colon wall during polyp removal. It is rare, occurring in about three to four per 10,Colonoscopy is the most widely used screening test for colon cancer, which is the second leading cause of cancer-related death in the United States. Credit: Illustration by The Epoch Times, Shutterstock colonoscopies. Symptoms may include fever, localized abdominal pain, and an increased white blood cell count.
Splenic Injury: This rare but potentially life-threatening complication can occur when the spleen is directly injured or torn by traction during the procedure. It typically causes pain in the upper left abdomen that may radiate to the left shoulder and can progress to low blood pressure and shock.
Infections: In rare cases, an infection may develop after a colonoscopy and require antibiotic treatment.
Cardiopulmonary events are related to the anesthesia or sedation used during colonoscopy. They can range from temporary issues such as low blood pressure, low oxygen levels, and fainting to more serious complications, including respiratory distress, irregular heartbeat, and acute coronary events.
Contact your doctor if you:
Have abdominal pain that does not improve after passing gas
Develop new or worsening abdominal pain
Feel nauseated or cannot keep fluids down
Notice blood in your stool
Develop a fever (100.4 F or higher)
Are unable to pass stool or gas
How Do I Prepare for a Colonoscopy?
“A successful colonoscopy hinges on a thoroughly cleansed colon, which is achieved through a standard preparation protocol involving dietary changes and a bowel-cleansing agent,” Lee-Kong said.
Special Diet: This bowel-cleaning process usually starts on the day before a colonoscopy. Lee-Kong recommends a low-fiber or clear liquid diet, while avoiding solid foods and red-colored liquids. Avoid fruit punch, cranberry juice, red wine, and red sports drinks. Medical professionals often advise avoiding red, orange, or purple foods and drinks, as the coloring can resemble blood or inflammation in the colon. Clear liquids commonly recommended the day before the procedure include black coffee, plain tea, fat-free broth, gelatin, clear sports drinks without added color, strained fruit juices, and water.
Bowel Preparation: This typically involves laxative solutions or tablets designed to fully cleanse the colon before the procedure. Patients are prescribed a laxative solution, often a polyethylene glycol (PEG) or sodium phosphate formula, to induce frequent bowel movements and clear the colon. The ‘split-dose’ method, where the solution is taken in two parts—the evening before and the morning of the procedure—is commonly recommended for a more effective cleanse, according to Lee-Kong. Other common options include sulfate-based solutions and magnesium citrate products.

